ACL (anterior cruciate ligament) tearA common injury of the knee is the tear of the anterior cruciate ligament (ACL), especially in „go-stop“ sports such as football, volleyball, handball, alpine skiing and dancing among others. An ACL injury leads to instability and stresses the joint structures, particularly the meniscus and cartilage. The knee looses its balance which causes a damaging shift toward to the medial motion center. Early development of cartilage defects and meniscus tears are the consequence. Physiotherapy, muscle - or coordination training cannot prevent the development of osteoarthritis.
Therefore, it is important in very active people who would like to return to their favourite sports to establish the necessary structural stabilisation in the knee joint. Which treatment is the best choice, has to be decided individually. |
Conservative treatment of ACL injuriesFor some less active people surgery is not the preferred choice for personal reasons. Physiotherapists offer treatment with a special proprioceptive training protocol in combination with advanced functional training. The mechanic and sensoric dysfunction needs to be compensated by muscles and other capsular structures. This, however, may overload other systems like the hip and the lower back, which in return leads to other disorders and defects.
A new sensomotoric training with the HUBER 360 helps to install a senso- and neuromuscular program to compensate the knee defect for sufficient stabilisation and function. If stabilisation cannot be achieved, surgical treatment has to be recommended to prevent knee osteoarthritis and further damages in the knee. |
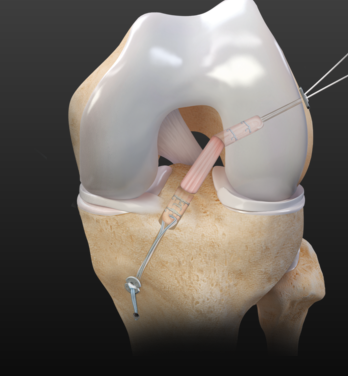
Biological ACL reconstruction using a small portion of the patellar tendon (PT) as graftThe classical and well proven procedure is the implant free, press-fit bone-tendon-bone reconstruction using a small strip of the medial part of patellar tendon. This anatomically precise technique uses the natural biological self-healing properties of tissue structures.
Fixation through a bone-to-bone healing offers a high grade of vitalisation, proprioception of the ligament and good neuromuscular control. No screws or other fixation aids, which could potentially disturb the healing process between the ligament and the bone, are used. The result is a fast, safe and stable bone-to-bone incorporation. The anatomically flat patella tendon stripe and the positioning of the bone-block rotation imitates the twist of a natural ACL during flexion and extension of the ligament. The result is a better internal stabilisation in flexion in comparison to other graft options. |
The design of the bone blocks has changed over the years to small blocks and a minimum of defect on the patella side at the extraction points. The defects are filled completely with bone material. Furthermore precise and careful harvesting of the medial part of the PT reduces pain disorders .Therefore, post surgery "anterior knee pain" could be reduced, comparable with other ACL reconstruction using other grafts.
All ideas of this technique enable early full weight bearing mobilisation within the first weeks after surgery. No knee orthesis is necessary. The anatomic PT technique is particularly well suited for physically active patients or high impact sports athletes. It may be the only technique for young women with hypermobility. Studies prove the technique's excellent long-term results in stability and full return to sports. |
Semi-biological ACL reconstruction using the quadriceps tendon (QT) as graftCurrently more knee surgeons are using a stripe of the quadriceps tendon for a semi-biological technique. Comparable to the "Patellar technique" a bone block from the Patellar, a middle strip of the quadriceps tendon and a screw for the tibial fixation come into use. Good results in fixation and endurance are reported. As a disadvantage, this technique may result in weakness of the quadriceps muscle in recovery. Therefore this procedure is not recommended in sports that require explosive power from the quadriceps muscle.
|

|
Healing response, a biological self-healing technique to preserve the ruptured ACL (using microfracturing)A complete ACL tear is rare. Most tears are incomplete and located close to the thighbone (femur). In this area of the ligament vascularisation and nerve connections are present. A thin skin wraps the ligament (synovial tube) and is often still intact. Therefore, in partial tears with a low degree of mechanical instability there is a real chance of re-adaption toward the femoral insertion. So, in some cases the ACL can heal without a surgery.
The current recommended approach is to stimulate the biological healing response through an arthroscopic procedure. Microfracturing creates small leaks in the insertion area of the ligament. This procedure helps the self-healing of the ligament with stem cells and additional growth factors from the patient's own bone marrow. Combined with a functional brace for external bracing and a sensomotorical training (HUBER 360) the results can be acceptable with less stress to the tissue and no damage from extraction of a donor tendon. Preconditions for this procedure are a young age, a partial (not complete) tear of the ACL, no other injuries and an early intervention within the first month after injury. Long-term studies of more than five years are not yet available, so not enough is known about the quality of the healed ACL ligament. However, good results have been seen in the first two years. |
ACL preserving technique
|
ACL reconstruction technique using the semitendinosus tendon (ST) as graftAn alternative method mostly used in Europe for low impact sports and lower levels of activity is an arthroscopic ACL reconstruction using the semitendinosus tendon (ST) from the hamstring muscles, which is fixated by small absorbable screws or pins. The use of the hamstrings may reduce explosive power in sprints and jumps (flexion power) and can result in hip disorders. The natural hamstring muscle system is important for stabilising the rotation and the translation in the knee, in the same way the hamstrings stabilizes the hip. The maturation of the ligament may be less effective as compared to the PT and QT ACL reconstruction. The neuromuscular control may remain weakened. Hence, patients undergoing this procedure require intensive rehab training. Post operative orthesis are recommended due to slow incorporation of the ligament into the bone tunnel. More and more studies show a rising number of loosening and re-ruptures a few years post reconstruction, especially in young patients and females. The hamstring technique may be recommended for athletes in low impact sports, but not in "contact" or "go and stop" sports.
|
|
